Dentistry in a post-COVID world
The “urgency of the now” is upon us and we must act together to help our patients
[ Words: John Marley ]
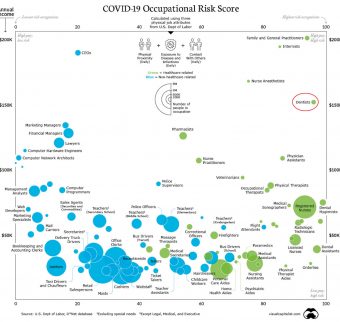
Dentistry and the patients it serves are in trouble. Occupational risk figures provided by the US Department of Labour suggest that in a post-COVID-19 (PC) world, dentistry is currently ranked very high risk.
Readers will be very well aware of the current financial and human impact on dentistry, as we have all suffered along with our patients over the past few months. It would be important at this time to draw out some potentially less recognised implications for the immediate and medium-term future. But to do so we must start, as always, with the patient.
The lack of services during this time, with the exception of rigidly controlled urgent dental care, means that there is already a sizeable cohort of patients with known disease awaiting treatment, in addition to those with disease yet to be diagnosed.
Our patients rely on several strands of dental service which work together to enable them to be seen and managed safely, efficiently, and effectively.
The first strand is an oncoming stream of undergraduate training, which has suffered enormously. While this year’s final years have been nudged towards the dental school exits with the “comfort blanket” of virtual examinations and the imprimatur of the respective Dental Councils, this cohort leaves with a sizeable professional development portfolio (PDP) of attainment work still to be met in their next phase of education as “safe beginners”.
For PDP read “IOU” and the problem arises that this particular IOU may not be easily cashed in as the GDP environment into which they enter will also be impacted.
The year behind will suffer more as they have not only lost around five months of clinical practice, but when they arrive back at their respective alma maters, they will be confronted by limited access to patients based on the exigencies of cross-infection control in the anxious PC world.
Dental schools themselves and their staff may be in jeopardy as most funding models will rely on a significant proportion of their undergraduate and postgraduate students being from overseas.
“These interventions will all demand willpower, unity of approach and,
of course, funding”
With the now well-described risk for those within the BAME community and the need to travel through a high-risk nexus of airports to get here; where COVID control is somewhat less advanced than many of their countries of origin, we may find that the current model will require significant university and Government financial support until the PC world has a cure or effective prevention for the virus.
The postgraduate training of these “safe beginners” is in jeopardy also. Access to patients and consequent attainments will necessarily be reduced and some may feel it better to postpone applications for PG courses and higher training until the smoke settles, thereby introducing a massive hole in future provision.
The situation is compounded further by the data from the latest Dental Schools Council report suggesting that up to 20 per cent of the senior teachers will be retiring imminently. As well as being treated safely, expertly, efficiently and effectively, patients expect to be treated in a timely fashion. In the PC world, waiting lists will significantly increase so current disease progresses and new disease goes undiagnosed for longer, creating a tsunami of issues for an already understrength dental service, especially as winter returns with the likelihood of a further surge. This is also compounded further by the missed appointments for those who would normally have been seen in the dental schools by students but now seek a GDP input.
Health services survived this time by “robbing Peter to pay Paul” and redeploying resources. However, with the demands of new and existing disease raising its head alongside a second surge or even just a chronic background of COVID, this may not be so easy the next time.
So what are the solutions?
It is noteworthy that the USA Department of Labour risk assessment figures (see graphic), notes the risks of CEOs (and presumably senior managers) to be low. It beholds all of those responsible for the oversight of dental services to understand each other and work co-operatively and without foot-dragging with those providing the service at the coal face, to ensure that expectations are managed and services attuned as best as possible to the anxious PC world.
Our patients deserve graduates, specialists and consultants who have appropriate training. This will require more, not less, human and general resources in the PC world. It will require:
Shift work extended over the day and over seven days of the week.
A funded programme to assist the PC graduate (and undergraduate) possibly increasing capacity through increase use of outreach into the “real world” of dentistry utilising available community poly clinic teaching or working co-operatively with larger multi-chair GDP practices generating income for them.
Funded, regulated and appropriate CPD provision to assist these PC graduates using everything we can, including radically improved clinical teaching laboratory access to remediate the effects of clinical deskilling.
Funded specialist and consultant training to provide a new generation of teachers and expert clinicians in their field in the PC world.
These (and more interventions like them) will all demand willpower, unity of approach and, of course, funding. The “urgency of the now” is upon us and we must act together.
John Marley BSc BDS PhD FDSRCS FDSRCS(Oral Surg) FFDRCSI is a Consultant Oral Surgeon in Belfast.